Thursday, July 06, 2006
Taking A Close Look At HepB
June 26, 2006
Filed under: in the news...
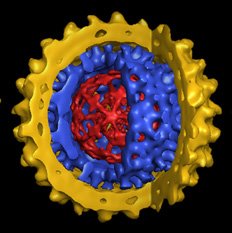
Using some of the latest investigational techniques, scientists at the Scripps Research Institute have discovered pretty amazing functional morphology of the Hepatisis B virus:
Hepatitis B virions, also known as Dane particles, are approximately 40 nanometers in size, and the capsid is surrounded by a membrane envelope. While the structure of the hepatitis B capsid has been studied intensively in vitro, until this study little was known about the structure and assembly of native capsids present in infected cells in vivo, and even less was known about the structure of mature virions.
"We used cryomicroscopy and image analysis to examine the native structure of HBV [hepatitis B virus ] capsids from transgenic mice and virions isolated from patient blood samples," Yeager said. [Mark Yeager, M.D., Ph.D. is a professor at Scripps -ed.] "By rapidly freezing the samples we were able to use cryo-electron microscopy to image the particles while they were maintained at the temperature of liquid nitrogen--around--300° F--which preserves them in a state close to what exists in vivo. Image processing allowed us to derive 3-D maps that revealed for the first time how the outer lipid envelope interacts with the capsid shell. "
The 3-D maps showed that in terms of molecular size, hepatitis B virus is enormous--nearly 10 times larger than a hemoglobin molecule. Like the human genome, the genome of the hepatitis B virus is formed by double-stranded DNA and enclosed by the capsid, which has icosahedral symmetry, resembling the geometric structure of a geodesic dome. The capsid itself is contained within an outer envelope formed by a lipid bilayer, similar to the membranes that enclose all human cells. The membrane of hepatitis B virus is studded with glycoprotein spikes, which bind to receptors on liver cells that mediate infection.
In hepatitis B-infected liver cells, transcription of the viral DNA produces a type of RNA that is packaged into capsids. Within the capsid, reverse transcription produces a single-strand DNA copy that serves as the template for second strand DNA synthesis. The resulting particles bud through membranes of the endoplasmic reticulum--the part of the cell involved with protein folding, assembly, and transport--to acquire the outer membrane envelope of the virus, a step that confers infectivity.
"In the transgenic mice, we found two types of capsids with different densities," Yeager said. "While both types of capsids were assembled as similar icosahedral structures, we found that the lower density capsids did not contain any viral DNA or viral RNA, while the higher density capsids contained viral DNA intermediates. It seems likely that these lower density capsids were released from the cell nucleus. These results may offer new clues how the virus replicates in vivo."
Statins Stop Hepatitis C Virus Replication ...

Japanese scientists say they've found statins, typically used as anti-cholesterol medications, can inhibit the replication of the hepatitis C virus.
The findings mean statins might be able to replace ribavirin in combination therapy with interferon. There are 170 million people worldwide infected with HCV. The standard HCV treatment is a combination therapy of interferon and ribavirin, which is effective in about 55 percent of patients. The remaining 45 percent face a threat of the disease progressing to cirrhosis and liver cancer. Aware of recent studies showing one statin, lovastatin, inhibits HCV replication, researchers led by Masanori Ikeda of Okayama University tested other statins in search of a more effective anti-HCV therapy. They evaluated the anti-HCV activities of five statins: atorvastatin, fluvastatin, lovastatin, pravastatin and simvastatin.
When the statins were tested alone, all except pravastatin inhibited HCV replication, with fluvastatin having the strongest effect; atorvastatin and simvastatin had moderate effects and lovastatin had a weak effect. The findings are reported in the July issue of the journal Hepatology.
Copyright 2006 by United Press International
Wednesday, July 05, 2006
Clinical Trials for Natural Hepatitis C Remedy Looking Good

June 28, 2006
What can interferon non-responders do about Hepatitis c? What about people who cannot or will not tolerate the devastating side effects of interferon therapy? Find out about the positive preliminary results from a medical study of a natural Japanese prescription medicine that's available to patients now.
Progressive Alternative Medicine Solution Undergoes Clinical Trials and Holds Promise of Benefiting Millions of Americans with Hepatitis CSource: HepCare Inc. Tuesday, May 23An estimated five million Americans have been infected with hepatitis C virus (HCV) according to a study published at the Liver Meeting by the American Association for the Study of Liver Diseases (AASLD) in November 2005. Chronic hepatitis C is associated with significant morbidity (liver cirrhosis and hepatocellular carcinoma) and mortality. Current treatment is based on interferon and ribavirin. However, treatment options are limited for patients who are not candidates for interferon-based therapy, particularly for those who suffer from HCV genotype 1 infection.
Sho-saiko-to (SST), a standardized herbal formula, is under a clinical phase II trial by a leading New York Cancer Research Institute to determine its effect on hepatitis C patients. The research group has reported the preliminary results of 15 patients at the 2nd Society of Integrative Oncology Conference in San Diego on November 10, 2005. This study is titled "Sho-saiko-to for Patients with Chronic Hepatitis C Who Are Intolerant to or Have Contraindication to Interferon-Based Therapy: A Phase II Study." SST is know to have anti-fibrotic effect by inhibition of lipid peroxidation in hepatocytes and stellate cells in animal studies. It has also been shown to reduce aminotransferase levels and the incidence of hepatocellular carcinoma in hepatitis and liver cirrhosis patients.
According to the design of the clinical trial, 31 patients will receive SST daily for 52 weeks. Fifteen patients have completed the treatment and the preliminary results have been reported. No serious adverse events have been attributed to SST among any patients who enrolled in the trial. Among the 15 patients who completed the study, reductions in alanine aminotransferase (ALT) were observed in 11 patients and aspartate aminotransferase (AST) in 10 patients. In 10 patients, the liver biopsy showed 20% improvement on histological assessment of the liver. This is consistent with the findings by the Japanese researchers for its anti-inflammatory effect. More interestingly, the majority of the patients whom participated in the clinical trial were genotype 1 infection.For more information about the herbal remedy, Sho-saiko-to, visit www.shosaikoto.com.
Monday, June 12, 2006
My doctor told me I am a "non-responder." What does that mean?

Hepatitis C treatment doesn't work for everyone. In some people, it works better than in others. If you are a non-responder, it means that your treatment didn't work as well as your doctor hoped that it would. There are many different kinds of "non-response." Some of the kinds that your doctor might mention include the following:
The treatment worked only as long as you took it. When you stopped taking it, hepatitis C came back.
Breakthrough response
The treatment seemed to work at first, but then it stopped working.
Partial response
The treatment seemed to work a little bit, but it never worked completely.
Hmmm, so what should you do, if your doctor feels that your
body can withstand tx.. Keep on trying.
Remember, I was labled a non-responder after 6 months
of mono-interferon and was told there was nothing else
I could do to rid my body of the HCV. I refused to be a victim
and found a doctor who believed in me and treatment. After doing
3 years of tx, I am Cured 8 years as of May 16, 2006.
So Please, do not give in or up!
Some Treatment Tips For Hepatitis C

I would like to say, I am far from being
an expert on Hepc, nor do I claim to be....
Trust me, I am not a Chatroom Doctor!
I'm just a sister that made it through her journey
and would like to help my fellow brothers & sisters
with their's!
You might say I was the "Poster Child for Interferon"
since it took me, 3 years of interferon injections
to become Virus Free, Hey I'm a blonde want do you want, lmao
I soon realized, not at first, that if I wanted,
to get well, I would have to be in charge!
So I gathered, as much information as
I could from the liver foundation,
because at the time, I did not have access to
the internet....
I would also prepare my questions for my doc
at home & wrote them down, because the treatment
was doing havoc with my memory.
I also joined Sherring Plough's "Be in Charge Program",
they sent me some information about Hepc,
that I found useful. They also assigned a nurse to me,
and she would call once a month, to see how I was doing.
That is great especially, if live by yourself,
at least you don't feel alone.
Most important tip, I can share is water, water,
water .... drink plenty of it!
Water helps to flush the toxic chemicals that we are
putting into our bodies.
After work, I would make it about about me!
I surrended my kitchen skills, lol and handed
them over to my family, or I ordered in!
I also assigned chores to my daughter, son
and husband. If they wanted me to get well....
Well, they would have to pitch in. Was tired of being
"Wonderwoman". I needed help, and
wasn't too proud to ask.
Most nights, you would find me on my couch,
listening to my favorite cd's. My husband bought me
a cd of nature sounds, that was that relaxing.
I always had the lights out, and surrounded myself
with candles and incense. Every Saturday,
I would go to the florist and buy myself some flowers.
I desperately needed to be surrounded by beauty,
since interferon was so very ugly!
For my achy, breaky, body I took lots & lots
of long bubble baths with mineral oils,
hmm that feels good! I also had an affair with my heating pad,
for three years! I'm happy to report that I ended that,
and me & hubby are back together, lol.
I also took tylenol or comtrex flu medicine
about 1/2 prior to injection to sort of get a jump start on the sides.
I ran a fever for three years, so this helped.
I found that by taking my injections between 7-8PM
that worked great for me, as soon as the
sides kicked in, I would take a sleeping pill,
and check out.
I decided to play with my calendar,
and started putting x's on my shot days.
When, my journey seemed endless, I would look at all
the x's and forcus on how many I already taken,
not how many I had ahead of me....
For my spiritual side, I was into meditation and
visualization, I would always see myself running
along the beach, laughing, and very healthy,
looking oh, so good with a great tan.
I felt if I believed that, I would be well,
just maybe I would.
I also kept a journal, for my inner most feelings.
I was undergoing so many emotions, and didn't
want to bother my family, with all, of what,
I was feeling. Besides they would have thought
I was nuts, lol ..
So, I expressed myself in writing, not in talking...
It felt great, to really express how I was feeling,
however, as I sometimes read my journals,
of which I have many, (three years worth)
I ask myself, hmm, now what was I thinking.
I did not suffer from serious depression.
When I felt, a little "out of my dish" I would remind myself,
that these thoughts were being induced by interferon,
and was not my thinking, it was the interferon. I was lucky,
that worked for me ....
However, many experience severe depression and
need anti-depressants, please inform your doc.
There are also some that have contemplated suicide,
please take this very serious and contact
your doc immediately.
Happy Trails to you!
If You Have HCV You Need Hope~

Hope is a word
that every
hurting heart
understands.
Hope shines
brighter than
the brightest star
on the darkest night.
Faith is bigger than the highest mountain.
And God is greater than any obstacle in your path.
Anything can be accomplished by those who fully
put their hearts into it. The time to start is now;
the place to start is
here. May hope
cast its special
light upon your
path and God
bless everything
you touch in the
hours, days,
and moments
still to come.
Is Working While You Have HCV The Right Decision?

If you're having major problems with fatigue, mental concentration, and other symptoms that are keeping you from holding a full-time job, a part-time job may seem to be a good solution. However, keep in mind that if you change your official job status from permanent full time to permanent part time, you may also change your insurance coverage, retirement plan, and other benefits. Company policies may be less flexible for part-timers than for full-timers. It may be difficult to switch back to full-time status. If your medical condition gets worse and you need to apply for Social Security Disability Insurance (SSDI), you may not qualify for full SSDI payments if your last permanent job was part time.
Be sure to find out all the details of part-time status from the human resource department before you make the switch. Perhaps you can arrange a temporary reduction in hours (and pay) that will let you keep your full benefits while you're recovering from hepatitis symptoms or treatment.
Can I use the Family Leave Act?
The Family Medical Leave Act (FMLA) says that if you have worked for your company full time for at least a year, you are allowed to take up to 12 weeks of unpaid time off every year (either on consecutive days or on an intermittent basis) to take care of your own serious medical needs. (Your spouse, child, or parent could also claim time under the FMNLA to take care of you if you are seriously ill.) If you return within 12 weeks or your period of absence does not exceed 12 weeks, under the Act your employer must give you your job (or an equivalent job) back when you return. Make sure you talk to your boss about the FMLA, and whether it applies to you, before you take the time off. Again, many states have laws which provide similar protection. For any particular situation you should consult a lawyer in your area.
If you think that your employer isn't willing to be as accommodating as you want in adjusting your workplace, you can contact the local office of the Equal Employment Opportunity Commission (EEOC), which handles ADA complaints, to look at your situation. (See the Resource List to find out how to contact the EEOC.)
You can also contact the Department of Justice, which operates the ADA Mediation Program. The Mediation Program provides federal mediators, or peacemakers, to try to work out such disagreements. (See the Resource List under the Americans with Disabilities Act Information Line to learn how to contact the Department of Justice in your region or the central office in Washington, D.C.) Every state has at least one mediator to step in and help. If that is not successful, you may still be able to sue under the provisions of the ADA.
Can I get disability payments?
Disability payments are often available under federal and state law. The U.S. government provides disability payments to people who have mental or physical problems that the government believes will keep them from being able to work at all. The Social Security Administration (SSA) has a list of conditions that it considers to be disabilities. If what you're experiencing is not on that list, you will have to prove to the SSA that you have a physical or mental condition that keeps you from being able to work.
Proving that you are disabled takes a lot of effort. You'll need proof of that from your doctor and supervisor, and possibly from some co-workers as well. You may also have to prove that you have tried different ways of working - perhaps doing a different job for the same employer, or adjusting your hours so that you can work when you feel best. The SSA may also want to know if you could work at a completely different job that is not as hard physically - say, instead of being a truck driver, if you could work as a dispatcher, or instead of being a teacher, if you could be a secretary. The SSA will want to know about other job skills you might have - if you have a home computer and can program computers, you might be encouraged to get a job doing that.
Do all you can to make it easy for the SSA workers to understand your situation by giving them complete information. It can be frustrating, but try to be patient with the process. It may take months for your case to work through the Social Security system. If you're asked to provide additional information, do so without delay. The time you waste is yours, not theirs!
Thursday, June 08, 2006
Zarqawi, Da Head Chopper Deader Than A Slab of Bacon....



US air strike kills Qaeda's Zarqawi
By Mariam Karouny 45 minutes ago
U.S. warplanes killed Abu Musab al-Zarqawi, the al Qaeda leader in Iraq blamed for bombings, beheadings and assassinations, in a strike which President George W. Bush said on Thursday had delivered justice.
In one of the most significant developments in Iraq since the capture of Saddam Hussein in 2003, Jordanian Zarqawi was killed in a bombing raid on Wednesday in a U-S.-Iraqi operation helped by tip-offs from Iraqis and Jordanian intelligence.
Vowing to fight on, al Qaeda in Iraq confirmed the death of Zarqawi, who beheaded several hostages himself and appeared in a recent video firing a machinegun in the desert.
U.S. forces displayed pictures to reporters of the corpse of the bearded Zarqawi with facial abrasions and his eyes closed. Wednesday's air strike was carried out by two F-16 planes with two 500 lb (227 kg) bombs hitting Zarqawi's "safe house."
Zarqawi, in his late 30s and whom Osama bin Laden called the prince of al Qaeda in Iraq, had symbolized the radical Islamist insurgency against U.S. occupation, and British Prime Minister Tony Blair said he now expected guerrillas to seek revenge.
"There will be fierce attempts ... with the death of Zarqawi to fight back," Blair said, adding the militant's death would not end the killing in Iraq but that it was significant.
A car bomb exploded in Baghdad on Thursday killing seven people just hours after Zarqawi's death was announced.
Bush said the death of Zarqawi, who had a $25 million bounty on his head, was "a severe blow to al Qaeda," a victory in the war on terrorism, and "an opportunity for Iraq's new government to turn the tide in this struggle."
GOVERNMENT BREAKTHROUGH
In a key political breakthrough, Iraq's parliament approved Prime Minister Nuri al-Maliki's candidates for new defense and interior ministers after intense wrangling among his coalition government partners.
Followers of Zarqawi, a Sunni Muslim who had declared war on Iraq's majority Shi'ites reinforcing fears he was out to ignite civil war, pledged to continue their fight.
"We tell our prince, Sheikh bin Laden, your soldiers in al Qaeda in Iraq will continue along the same path that you set out for Abu Musab al-Zarqawi," said a statement on an Islamist Web site. "The death of our leaders ... only makes us more determined to continue the jihad."
Maliki, who was desperately in need of success to bolster his authority, announced Zarqawi's death near the city of Baquba 65 km (40 miles) north of the capital.
Bush said U.S. special forces confirmed Zarqawi's location based on intelligence from Iraqis and "delivered justice to the most wanted terrorist in Iraq."
"It truly was a very long, painstaking, deliberate exploitation of intelligence, information gathering, human sources, electronics, signal intelligence," U.S. Major General William Caldwell said, adding the operation took many weeks.
U.S. forces were trailing Sheikh Abdul-Rahman, Zarqawi's spiritual adviser, and that led them to a small house in a palm grove area and Zarqawi.
Six people, including a woman and a child, were killed in the house but only Zarqawi and Abdul-Rahman have been identified. Zarqawi was identified by his fingerprints and tattoos. A further DNA test was being carried out on Zarqawi.
BAGHDAD RAIDS
Seventeen raids were launched on suspected hideouts for Zarqawi associates in the Baghdad area hours after he was killed. They produced a "treasure trove" of information, officials said.
Zarqawi's death had an impact on oil prices. Crude futures were down more than one dollar to $68.17 a barrel.
Zarqawi, who U.S. Ambassador Zalmay Khalilzad called the "godfather of sectarian killing in Iraq" and who faced four death sentences in Jordan, one for his role in killing a U.S. diplomat, had inspired a flood of militants from across the Arab world to blow themselves up in suicide missions.
Taunting Bush during the video taped killing of a sobbing, blindfolded U.S. hostage, Zarqawi once boasted his al Qaeda fighters "love death just like you love life."
"Killing for the sake of God is their best wish," the insurgent leader said, drawing a knife to hack off the head of his kneeling victim.
Zarqawi's reputation for personal savagery stood out even in a country where brutal killings were routine, and sparked reports bin Laden and his deputy Ayman al-Zawahri were worried his homicidal zeal would undermine support for their network.
"His whole intent was to incite violence between Shi'ites and Sunnis. He wasn't interested in going after coalition forces," said Caldwell of the former street thug who had eluded repeated attempts to capture or kill him.
Some Arab citizens hailed Zarqawi as a hero for his role in the insurgency but others welcomed his death as a form of justice for a militant whose attacks killed far more Iraqi civilians than foreign troops.
Caldwell said an Egyptian militant trained in Afghanistan called Abu al-Masari, who established the first al Qaeda cell in Baghdad, may succeed Zarqawi as head of the group in Iraq.
My thanks To Our Us Military.... God Bless You.
Tuesday, June 06, 2006
Relative Risks Of Cirrhosis From Non-alcoholic Steatohepatitis

Main Category: Liver Disease / Hepatitis News
Article Date: 06 Apr 2006 - 3:00am (PDT)
Cirrhosis related to non-alcoholic steatohepatitis (NASH) is associated with fewer complications and a lower mortality compared to cirrhosis from hepatitis C, despite NASH patients' greater risk of dying from cardiovascular events. These findings are published in the April 2006 issue of Hepatology, the official journal of the American Association for the Study of Liver Diseases (AASLD). Published on behalf of the society by John Wiley & Sons, Inc., Hepatology is available online via Wiley InterScience at http://www.interscience.wiley.com/journal/hepatology.
Non-alcoholic steatohepatitis can develop as a consequence of obesity and the metabolic syndrome. It is considered a "silent" disease, with most sufferers feeling well, in spite of inflammation and damage to the liver. But NASH can progress to cirrhosis in up to 20 percent of cases. With obesity becoming more prevalent in the U.S., the health care burden related to cirrhosis due to NASH is expected to rise. Up to now, however, little has been known of the natural history of cirrhosis associated with NASH.
Researchers led by Arun J. Sanyal, M.D. of Virginia Commonwealth University Medical Center in Richmond, sought to prospectively define the clinical outcomes of cirrhosis due to NASH, and compare them to those associated with hepatitis C virus (HCV) infection. They studied 152 patients with cirrhosis due to NASH and matched them with 150 patients with cirrhosis due to HCV. For each participant, the researchers collected information on mortality and morbidity, including synthetic failure, varices and variceal hemorrhage, ascites, encephalopathy and hepatocellular cancer.
Over ten years, 29 of the 152 subjects with cirrhosis due to NASH died, compared to 44 of the 150 subjects with cirrhosis due to HCV. Sepsis was the most common cause of death in both groups and was often associated with acute or chronic liver failure.
At the same time, cardiac events killed many more patients with NASH (8 out of 152) than with HCV (1 out of 150) a finding that is "noteworthy, although not unexpected," report the authors. "This group has significantly higher prevalence of risk factors for coronary heart disease and congestive heart failure than those with HCV." During the study, patients with cirrhosis due to NASH and normal liver functions developed fewer complications of cirrhosis: 14 NASH patients developed ascites, compared to 40 HCV patients. Also, fewer NASH patients than HCV patients developed encephalopathy and variceal hemorrhage, and significantly fewer developed liver cancer. However, once the liver functions declined below normal levels, the outcomes of patients with NASH were the same as those with cirrhosis from hepatitis C.
"These are the first prospective data on the relative risks of developing specific complications of cirrhosis in subjects with NASH," the authors report. NASH patients fared better overall compared to HCV patients, though many did develop complications of cirrhosis. Ascites was the most common complication contributing to mortality.
"These data are likely to be important in the design of future therapeutic interventions in this patient population," the authors conclude, "and also in the everyday management of such patients in clinical practice."
Article: "Similarities and Differences in Outcomes of Cirrhosis Due to Nonalcoholic Steatohepatitis and Hepatitis C," Arun J. Sanyal, Colin Banas, Carol Sargeant, Velimer A. Luketic, Richard K. Sterling, Richard T. Stravitz, Mitchell L. Shiffman, Douglas Heuman, Adrian Cotterell, Robert A. Fisher, Melissa J. Contos, and Alan S. Mills, Hepatology; April 2006 (DOI: 10.1002/hep.21103).
David Greenberg
dgreenbe@wiley.com
John Wiley & Sons, Inc.
DEALING WITH PRE-TREATMENT WORRIES....
 A person who is about to begin treatment with interferon, will likely be concerned about its potential side effects. This is understandable. After all, many people with hepatitis C feel fine, so it’s perfectly normal to worry about starting a medication that may make them feel sick. Alternatively, some people with hepatitis C already feel run down as a result of the virus. The last thing that these individuals want to do is to begin a medication that may make them feel even worse.
A person who is about to begin treatment with interferon, will likely be concerned about its potential side effects. This is understandable. After all, many people with hepatitis C feel fine, so it’s perfectly normal to worry about starting a medication that may make them feel sick. Alternatively, some people with hepatitis C already feel run down as a result of the virus. The last thing that these individuals want to do is to begin a medication that may make them feel even worse.Side effects associated with any drug, including interferon, vary from person to person. This means that not everyone will experience a particular potential side effect. So, while some individuals feel quite ill while on interferon, others experience few, if any, side effects. And there are some individuals who actually feel better while on interferon. That’s right! This point bears repeating. It is a possibility that a person will have minimal to no side effects, or will even feel better than usual while on interferon. And, those that do experience adverse side effects usually do not experience them all the time. In fact, studies have shown that, only approximately two- to -five percent of people find the side effects of interferon so debilitating that discontinuation of therapy is necessary.
SOME GENERAL POINTS TO KEEP IN MIND
It is important to do everything you can to minimize the side effects of interferon therapy. Your objective should be to make sure that the side effects of interferon do not cause the discontinuation of therapy. Side effects of interferon therapy are usually the worst during the first few weeks of therapy. So, it’s important to try to stick with therapy for at least a month or two.
It typically takes the body this initial period of time to adjust to interferon. So, don’t assume that the way you feel after the first injection is the way you will feel every time you inject. Some people schedule time off from work for when they plan to start interferon therapy. Or, they begin therapy during their vacation week. Others plan to begin therapy when their work schedule or personal responsibilities are light, thereby making it is easier to get through the initial period.
If side effects become too severe, don’t be afraid to ask your doctor to help you apply for temporary disability. Lastly, always keep in mind that the side effects due to interferon will totally abate after interferon therapy has been discontinued
Definition of HCV PCR

HCV PCR: HCV PCR (polymerase chain reaction) is a test for the hepatitis C virus (HCV).
There are three types of HCV PCR tests:
The HCV PCR viral detection test: This qualitative test is designed to detect whether the hepatitis C virus is or is not present.
The HCV PCR viral load test: This quantitative test looks for the virus and estimates the number of HCV viruses per ml of blood.
The HCV PCR genotype test: This test looks for the virus and determines the particular subtype of HCV.
The three different HCV PCR tests serve different purposes. The qualitative test is done to confirm the presence of HCV in the blood of a person with positive HCV antibody test. The quantitative test is done to estimate the length of treatment that will be needed and to monitor the effectiveness of that treatment. The genotype test is usually done before the start of treatment because it can differentiate each of the major subtypes of HCV. Knowing the subtype can be important because, for example, treatment with interferon is more often effective for people with genotype subtypes 2 or 3 than for those with genotype 1.
Chronic VS. Acute Hepatitis C infection

Acute Hepatitis C infection is the period of time that begins with the intial infection, and includes the incubation period and the possible appearance of clinical illness. Because the hepatitis C virus has the ability to evade the immune response in many people, about 85 percent of patients with acute HCV infection develop persistent infection. Chronic hepatitis C, defined as persistently elevated alanine aminotransferase (ALT) levels more than 6 months after illness onset, develops in about 70 percent of cases.
Symptoms of Acute HCV Infection
Not everyone infected with the hepatitis C virus has symptoms of infection. Studies have shown that 60 to 70 percent of patients with acute HCV infection have no discernable symptoms. Approximately 20 to 30 percent of patients may be ill with jaundice. About 10 to 20 percent of acutely infected people have vague and non-specific symptoms that can be can be easily mistaken for other illnesses. When present, symptoms have been described as "flu-like" and can include: Fatigue: a feeling of weariness of exhaustion. Liver pain: discomfort or tenderness in the upper right quadrant of the abdomen, which may be associated with enlargement of the liver .Nausea and decreased appetite,
Pain in muscles and joints.
When patients with acute HCV infection seek medical attention, about 80 percent have elevated levels of bilirubin and alanine aminotransferase (ALT). Only about 15 percent of patients require hospitalization. In rare cases, HCV infection can cause fulminant hepatic failure. This complication is more likely to occur when patients have other diseases that impair their immune systems, such as HIV, or have pre-existing liver disease.
HCV Incubation and the Appearance of Symptoms
Incubation is the period of time between exposure and infection, and the manifestation of the disease. The incubation period for newly acquired acute hepatitis C ranges from two weeks to six months, with an average incubation period of six to seven weeks. Blood tests can detect the presence of the HCV virus in blood after 1 to 3 weeks of infection. By the time symptoms appear, 70 to 80 percent of patients have detectable antibodies to HCV. HCV antibodies can be detected in about 90 percent of infected people by 3 months after the appearance of symptoms. Ultimately, HCV antibodies become detectable in over 95 percent of HCV-infected persons. Although the period of acute HCV infection is variable, one of the more prominent characteristics features is fluctuating blood levels of alanine aminotransferase, sometimes by hundreds of units per week. Over time, ALT levels can return to normal, but may later be followed by prolonged, symptomless ALT elevations indicating active chronic disease.
Treating Obesity May Improve The Efficacy Of Therapy For Hepatitis C
Main Category: Liver Disease / Hepatitis News
Article Date: 03 Jun 2006 - 0:00am (PDT)
According to a new study, obese patients chronically infected with the hepatitis C virus (HCV) and treated with combination drug therapy may have better outcomes if the underlying abnormalities caused by excessive fat tissue are corrected. Weight loss, medications to decrease insulin resistance and extending duration or dosage of therapy are strategies that may improve the efficacy of therapy.
The results of this study appear in the June 2006 issue of Hepatology, the official journal of the American Association for the Study of Liver Diseases (AASLD). Published by John Wiley & Sons, Inc., Hepatology is available online via Wiley InterScience at http://www.interscience.wiley.com/journal/hepatology.
HCV is one of the leading causes of chronic liver disease worldwide, affecting 3 percent of the world's population. In the U.S. alone 4.1 million people have been infected with HCV, and up to 85 percent of those are chronic carriers of the virus. Up to 70 percent of chronic carriers will go on to develop some other form of chronic liver disease, from mild liver enzyme abnormalities to cirrhosis and liver cancer. While there is no vaccine for HCV, the current optimal treatment is combination therapy with peginterferon alfa (an immune stimulant) and ribavirin (an inhibitor of viral replication). However, this will cure only 55 percent of patients. One of the risk factors for treatment failure is obesity.
Obesity itself is linked to the disruption of hormone signaling pathways that affect cell function and to abnormal levels of circulating proteins and sugars. In other words, obesity is associated with a wide range of metabolic changes that affect multiple cellular and organ functions. This biochemical disregulation is linked to serious chronic medical conditions, such as heart disease, diabetes, and non-alcoholic fatty liver disease.
Given the association between obesity and metabolic abnormalities, Michael R. Charlton, M.D. of the Division of Gastroenterology and Hepatology at the Mayo Clinic and Foundation in Rochester, MN and coauthors reviewed several mechanisms by which obesity may interfere with the treatment of chronic HCV and recommend management strategies for obese patients.
The authors identify three possible ways by which obesity may interfere with peginterferon alpha and ribavirin activity. First, fat tissue actively secretes hormones that can modulate the immune system. Increases in fat tissue may disregulate immune pathways peginterferon targets, rendering the drug ineffective. Second, obesity causes insulin resistance which itself leads to the accumulation of fat in the liver. The greater the accumulation of fat in the liver, the greater the risk of fibrosis, or scar tissue formation, that alters liver function and blood flow, often permanently. Because HCV also causes liver cells to not respond to insulin, obesity may simply compound the problem and worsen liver disease. Third, fat tissue reduces the amount of peginterferon circulating in the body. The decreased circulation of the drug may also weaken peginterferon's stimulation of the immune system against HCV.
To address all of these mechanisms, the authors make three treatment recommendations. First, weight loss to reduce fat tissue would address all three hypothesized mechanisms. Weight loss in obese HCV patients is already associated with improved liver biopsy results and liver enzyme levels. Second, treatment with drugs that improve cellular sensitivity to insulin, such as the diabetes drugs metformin or pioglitazone, would lead to reduced fat accumulation in liver cells and might reverse disease progression. Third, increasing the dosages or the duration of combination therapy may increase circulating drug levels and improve drug efficacy.
"Treatment strategies that focus on improving underlying metabolic factors associated with poor response to combination therapy are thus more likely to overcome the low sustained viral response rates often observed in obese patients infected with HCV," conclude the authors.
David Greenberg
dgreenbe@wiley.com
John Wiley & Sons, Inc.
http://www.interscience.wiley.com/
Diabetes Link to Liver Disease...

Most patients with diabetes know that they have an increased risk of heart disease and stroke, but few realize that their diabetes is also raising their risk of having both liver disease and liver cancer. "There is now growing evidence that some endocrine disorders, in particular diabetes mellitus, may actually cause liver disease." said Dr. Adrian M. DiBisceglie of the division of gastroenterology and hepatology at the Saint Louis University School of Medicine in a response to the new data. A pair of studies reveal that patients with type 2 diabetes have two times the risk of developing liver disease and possibly three times the risk of developing liver cancer as their healthy peers.
Because liver disease can go undetected for years, these findings emphasize the importance for those with diabetes to keep a close eye on their liver health.
Reviewing the Problem
In the first study, published in Gastroenterology, researchers followed over 170,000 patients with type 2 diabetes and over 650,000 patients without diabetes who were admitted to various VA hospitals across the country. Fifteen years after being discharged, the patients with diabetes were almost twice as likely to have chronic liver disease as the patients without diabetes.
While it is unclear whether diabetes directly causes liver disease, or if changes in liver function cause diabetes, Dr. Hashem El-Serag, study author from the Houston Veteran Affairs Medical Center, sees this study as an important warning for patients with diabetes. Because liver disease can often go unnoticed, as it causes no discernible symptoms, he recommends "regular testing of liver enzymes for patients with diabetes."
In a related study, published in the journal Gut, 2,061 patients with liver cancer were compared to over 6,000 patients without liver cancer from a Medicare database. The researchers found that 43 percent of the patients with liver cancer also had diabetes, while only 19 percent of the cancer-free control group had diabetes. When other factors that contribute to liver cancer risk, like alcoholism, were taken into account, the researchers found that patients with diabetes had three times the risk of developing liver cancer as the general population.
"Our results indicate that diabetes is associated with an increased risk of [liver cancer] among people 65 years and older." wrote El-Serag.
Chronic liver diseases, caused by hepatitis B, hepatitis C, heavy alcohol consumption and fatty liver disease have previously been shown to be major risk factors for developing liver cancer, but this is the first time that diabetes alone was seen as a risk factor for liver cancer. This correlation may explain why rates of liver cancer have been on the rise in the United States.
"The incidence of liver cancer is rising in the developed Western world at a time when obesity is also emerging as a major public health threat." said DiBisceglie. "What is the link between these two phenomena?"
© 2006 Healthology, Inc.
Can you have a "false positive" anti-HCV test result?
Yes. A false positive test means the test looks as if it is positive, but it is really negative. This happens more often in persons who have a low risk for the disease for which they are being tested. For example, false positive anti-HCV tests happen more often in persons such as blood donors who are at low risk for hepatitis C. Therefore, it is important to confirm a positive anti-HCV test with a supplemental test as most false positive anti-HCV tests are reported as negative on supplemental testing. Click here for more information on Guidelines for Laboratory Testing and Result Reporting of Antibody to Hepatitis C Virus.
Can you have a "false negative" anti-HCV test result?
Yes. Persons with early infection may not as yet have developed antibody levels high enough that the test can measure. In addition, some persons may lack the (immune) response necessary for the test to work well. In these persons, research-based tests such as PCR may be considered.
How long after exposure to HCV does it take to test positive for anti-HCV?
Anti-HCV can be found in 7 out of 10 persons when symptoms begin and in about 9 out of 10 persons within 3 months after symptoms begin. However, it is important to note that many persons who have hepatitis C have no symptoms.
How long after exposure to HCV does it take to test positive with PCR?
It is possible to find HCV within 1 to 2 weeks after being infected with the virus.
Who should get tested for hepatitis C?
persons who ever injected illegal drugs, including those who injected once or a few times many years ago persons who were treated for clotting problems with a blood product made before 1987 when more advanced methods for manufacturing the products were developed persons who were notified that they received blood from a donor who later tested positive for hepatitis C persons who received a blood transfusion or solid organ transplant before July 1992 when better testing of blood donors became available long-term hemodialysis patients persons who have signs or symptoms of liver disease (e.g., abnormal liver enzyme tests) healthcare workers after exposures (e.g., needle sticks or splashes to the eye ) to HCV-positive blood on the job children born to HCV-positive women
What is the next step if you have a confirmed positive anti-HCV test?
Measure the level of ALT ( alanine aminotransferase, a liver enzyme) in the blood. An elevated ALT indicates inflammation of the liver and you should be checked further for chronic (long-term) liver disease and possible treatment. The evaluation should be done by a healthcare professional familiar with chronic hepatitis C.
Can you have a normal liver enzyme (e.g., ALT) level and still have chronic hepatitis C? Yes. It is common for persons with chronic hepatitis C to have a liver enzyme level that goes up and down, with periodic returns to normal or near normal. Some persons have a liver enzyme level that is normal for over a year but they still have chronic liver disease. If the liver enzyme level is normal, persons should have their enzyme level re-checked several times over a 6 to 12 month period. If the liver enzyme level remains normal, your doctor may check it less frequently, such as once a year.
Monday, June 05, 2006
Reliable early prediction of viral relapse
Reliable early prediction of viral relapse by detection of minimal residual hepatitis C viremia at treatment week 12
DDW, Los Angeles, May 21-24, 2006 (Digestive Disease Week)
A. Bergk1; C. Sarrazin2; M. von Wagner2; G. Teuber3; P. Buggisch4; V. Weich1; B. Wiedenmann1; T. Berg1
1. Hepatology and Gastroenterology, Charite, CVK, Berlin, Germany.
2. Internal Medicine II, Universitaetsklinikum des Saarlandes, Homburg, Germany.
3. Internal Medicine II, UniversitaetsklinikumFrankfurt, Frankfurt am Main, Germany.
4. Center for Internal Medicine, Universitaetsklinikum Hamburg, Hamburg, Germany.
Introduction: Current treatment guidelines for the therapeutic management of chronic hepatitis C virus (HCV) genotype 1 infected patients include a week 12 stopping rule for nonresponders defined by a drop of viral load less than 2 log10 in patients treated with pegylated interferon and ribavirin. Nevertheless there has been no convincing prognostic tool to easily and reliably predict viral relapse after the end of 48 weeks of treatment.
Aims: Aim of the present study was to evaluate the predictive value of a minimal residual HCV viremia for a relapse in genotype 1 infected patients with early virologic response to therapy.
Patients and methods: We retrospectively analyzed viral kinetics at week 12 and response of 773 treatment naive HCV genotype 1-infected patients using PegIFNα-2a/b and ribavirin treated at our outpatient clinics. For the detection of residual viremia at week 12 a quantitative real-time PCR with a lower limit of detection of 10IU/mL (TaqMan) was used.
Results: Using standard quantitative HCV-RNA assays at week 12 75% (430/773) of the patients treated with PegIFNα-2a/b and ribavirin showed an early virologic response defined by week 12 viral load drop ≥2 log10. By re-analyzing 222 available serum samples of early virologic responders by TaqMan a residual viremia could be detected in 84 out of 222 patients (38%). The presence of viremia highly correlated with a viral relapse after the end of 48 weeks of treatment (p<0,001).>
A relapse occurred in 78% of the patients who had detectable HCV viremia at week 12 (68/88) as compared to only 19% (25 out of 134 patients) if HCV RNA was undetectable at week 12. The relative risk to suffer from a relapse was 3.5 and 0.26 in patients with and without residual hepatitis C viremia at week 12, respectively (p<0,001).>Discussion: Using a highly sensitive real-time PCR the detection of minimal residual hepatitis C viremia at treatment week 12 was in 78% associated with a viral relapse after the end of therapy and is therefore a valuable prognostic tool for the prediction of individual treatment outcome. Treatment of patients with detectable viremia at week 12 should be individually intensified by either prolonging treatment duration or preventing dose reductions by the application of erythropoetin or GM-CSF.
Noninvasive determination of HCV or other infectious liver disease
The BreathID® system is unique in many ways. It is able to diagnose and monitor a multitude of functional GI and internal disorders through testing applications such as Helicobacter pylori, Liver Function and Gastric Emptying Rate. The system is ideal for a wide range of patients that suffer from functional dyspepsia, diabetes, Parkinson's disease, a wide range of liver diseases such as Hepatitis (HCV, HBV), NAFLD, NASH diseases, and those related to alcoholism. The BreathID's remarkable benefits and unbeatable performance are a result of its unique and proprietary technologies: Microstream®, MCS™ (Molecular Correlation Spectroscopy) and CRT (Continuous Real Time) technology on-line analysis algorithms. These advantages include automatic operation, immediate test results, the shortest possible testing times, no need for active patient cooperation and more clinical information in each measurement due to the continuous sampling.
http://archive.mail-list.com/hbv_research/msg09603.html
Noninvasive determination of HCV or other infectious liver disease
The Oridion BreathID®
Filed under: Diagnostics , GI , Medicine
The Jerusalem Post is reporting that an instrument manufactured by Oridion Systems Ltd. can noninvasively determine whether a patient has hepatitis C or some other infectious liver disease, with the results available in 40 minutes or so.
The instrument is named Oridion BreathID® and the description of it as follows:
The BreathID® system is unique in many ways. It is able to diagnose and monitor a multitude of functional GI and internal disorders through testing applications such as Helicobacter pylori, Liver Function and Gastric Emptying Rate. The system is ideal for a wide range of patients that suffer from functional dyspepsia, diabetes, Parkinson's disease, a wide range of liver diseases such as Hepatitis (HCV, HBV), NAFLD, NASH diseases, and those related to alcoholism.
State-of-the-Art Technology and Design for Every Environment
The BreathID's remarkable benefits and unbeatable performance are a result of its unique and proprietary technologies: Microstream®, MCS™ (Molecular Correlation Spectroscopy) and CRT (Continuous Real Time) technology on-line analysis algorithms. The use of these technologies enables BreathID® to offer several distinct advantages over other testing systems and methods. These advantages include automatic operation, immediate test results, the shortest possible testing times, no need for active patient cooperation and more clinical information in each measurement due to the continuous sampling.
BreathID® was designed with the needs of both the physician/operator and the patient in mind. Simple single-button operation, self-calibration and a user-friendly interface enable easy test administration by any member of the staff with no need for prior training or orientation.
http://www.medgadget.com/archives/2006/05/the_oridion_bre.html
Alternative Medicine Solution Undergoes Clinical Trials and Holds Promise of Benefiting Millions of Americans with Hepatitis C
Sho-saiko-to (SST), a standardized herbal formula, is under a clinical phase II trial by a leading New York Cancer Research Institute to determine its effect on hepatitis C patients. This study is titled "Sho-saiko-to for Patients with Chronic Hepatitis C Who Are Intolerant to or Have Contraindication to Interferon-Based Therapy: A Phase II Study." SST is know to have anti-fibrotic effect by inhibition of lipid peroxidation in hepatocytes and stellate cells in animal studies. It has also been shown to reduce aminotransferase levels and the incidence of hepatocellular carcinoma in hepatitis and liver cirrhosis patients.
According to the design of the clinical trial, 31 patients will receive SST daily for 52 weeks. Fifteen patients have completed the treatment and the preliminary results have been reported. No serious adverse events have been attributed to SST among any patients who enrolled in the trial. Among the 15 patients who completed the study, reductions in alanine aminotransferase (ALT) were observed in 11 patients and aspartate aminotransferase (AST) in 10 patients. In 10 patients, the liver biopsy showed 20% improvement on histological assessment of the liver. More interestingly, the majority of the patients whom participated in the clinical trial were genotype 1 infection.
http://www.transworldnews.com/NewsStory.aspx?storyid=8446&ret=Default.aspx
Progressive Alternative Medicine Solution Undergoes Clinical Trials and Holds Promise of Benefiting Millions of Americans with Hepatitis C
PHOENIX 5/23/2006 7:46 PM GMT (TransWorldNews) An estimated five million Americans have been infected with hepatitis C virus (HCV) according to a study published at the Liver Meeting by the American Association for the Study of Liver Diseases (AASLD) in November 2005. Chronic hepatitis C is associated with significant morbidity (liver cirrhosis and hepatocellular carcinoma) and mortality. Current treatment is based on interferon and ribavirin. However, treatment options are limited for patients who are not candidates for interferon-based therapy, particularly for those who suffer from HCV genotype 1 infection.
Sho-saiko-to (SST), a standardized herbal formula, is under a clinical phase II trial by a leading New York Cancer Research Institute to determine its effect on hepatitis C patients. The research group has reported the preliminary results of 15 patients at the 2nd Society of Integrative Oncology Conference in San Diego on November 10, 2005. This study is titled "Sho-saiko-to for Patients with Chronic Hepatitis C Who Are Intolerant to or Have Contraindication to Interferon-Based Therapy: A Phase II Study." SST is know to have anti-fibrotic effect by inhibition of lipid peroxidation in hepatocytes and stellate cells in animal studies. It has also been shown to reduce aminotransferase levels and the incidence of hepatocellular carcinoma in hepatitis and liver cirrhosis patients.
According to the design of the clinical trial, 31 patients will receive SST daily for 52 weeks. Fifteen patients have completed the treatment and the preliminary results have been reported. No serious adverse events have been attributed to SST among any patients who enrolled in the trial. Among the 15 patients who completed the study, reductions in alanine aminotransferase (ALT) were observed in 11 patients and aspartate aminotransferase (AST) in 10 patients. In 10 patients, the liver biopsy showed 20% improvement on histological assessment of the liver. This is consistent with the findings by the Japanese researchers for its anti-inflammatory effect. More interestingly, the majority of the patients whom participated in the clinical trial were genotype 1 infection.
In Japan, over 75% of physicians use at least some of the traditional herbal formulas. Over 1.5 million Japanese patients with hepatitis have been treated with Sho-saiko-to. SST is available in capsules through HepCare Inc. (www.HepZone.com), a Phoenix-based company that has licensed the marketing right of SST from Honso Pharmaceutical Co. Ltd., the Nagoya-based Japanese manufacturer of the standardized herbal formula.
For more information about SST, please visit www.HepZone.com, call 800-996-4SST (778) or e-mail info@hepzone.com.
HepZone(R) is a registered trademark of HepCare Inc., 4602 E. Elwood St., Suite 6, Phoenix, AZ 85040.
HepCare Inc., Phoenix
Jennifer Healy, 800-996-4778
Wednesday, May 31, 2006
CIFN Has Much Higher Biological Activity Than PegIFN
Unlike alfa and beta interferons, which are naturally occurring interferons, consensus interferon is a recombinant type 1 interferon that was derived by scanning sequences of naturally occurring alfa interferon and adding the most frequently observed amino acid in each corresponding position. As a result CIFN has much higher biological activity than pegIFN so it "adheres to the virus cell more tightly than pegIFN," said Dr. Kaiser.
Daily consensus interferon plus Rebetol (ribavirin) for 72 weeks produced sustained viral response in 70% of patients with chronic hepatitis C who became refractory to Rebetron (pegylated interferon alfa 2a plus ribavirin), according to a pilot study reported here.
CIFN was given as a daily injection (9 ìg) and pegIFN (180 ìg) was given once a week. Patients in both treatment arms received weight-based Rebetol. At the end of 72 weeks the viral response was confirmed in 89% of the patients in the CIFN arm and in 76% of patients treated with pegIFN (NS). Although the CIFN was generally well tolerated, there were more injection site reactions in the CIFN arm and there was slightly higher drop-out rate in the CIFN treatment group, 18% versus 12% for the pegIFN group. When you have this sustained viral response, that's a 99% chance of a cure," Dr. Vierling said. "That's very impressive." The next step, he said, would be to confirm the results in a larger study. http://www.medpagetoday.com/InfectiousDisease/Hepatitis/dh/3357
DDW: Relapsed HCV Patients Achieve Sustained Response with 72-Week Treatment
By Peggy Peck, MedPage Today Staff Writer
Reviewed by Rubeen K. Israni, M.D., Fellow, Renal-Electrolyte and Hypertension Division, University of Pennsylvania School of Medicine
May 22, 2006
MedPage Today Action Points
Explain to interested patients that these results were based on a small study and the findings need to be confirmed in a larger clinical trial. Explain to patients who ask that consensus interferon treatment requires daily injections. This study was published as an abstract and presented in a poster at a conference. These data and conclusions should be considered to be preliminary as they have not yet been reviewed and published in a peer-reviewed publication
Review:Stephan Kaiser, M.D.
University of Tuebingen
LOS ANGELES, May 22 — Daily consensus interferon plus Rebetol (ribavirin) for 72 weeks produced sustained viral response in 70% of patients with chronic hepatitis C who became refractory to Rebetron (pegylated interferon alfa 2a plus ribavirin), according to a pilot study reported here. The findings, presented at Digestive Disease Week sessions, compared consensus interferon (CIFN) plus Rebetol with pegylated interferon alfa 2a (pegIFN) plus Rebetol in 81 patients who relapsed after 48 weeks of treatment with Rebetron and found that extending treatment to 72 weeks resulted in good response in both treatment arms, said Stephan Kaiser, M.D., of the University of Tuebingen in Germany. But sustained response was significantly better in the CIFN group with 69% of those patients remaining virus-free for at least four months after completing treatment, versus a 44% sustained viral response rate in the pegIFN arm (P<0.05).>
At the end of 72 weeks the viral response was confirmed in 89% of the patients in the CIFN arm and in 76% of patients treated with pegIFN (NS). Although the CIFN was generally well tolerated, there were more injection site reactions in the CIFN arm and there was slightly higher drop-out rate in the CIFN treatment group, 18% versus 12% for the pegIFN group. John Vierling, M.D., president of the American Association for the Study of Liver Diseases and professor of medicine at Baylor in Houston, was enthusiastic about the results. "When you have this sustained viral response, that's a 99% chance of a cure," Dr. Vierling said. "That's very impressive." The next step, he said, would be to confirm the results in a larger study. Unlike alfa and beta interferons, which are naturally occurring interferons, consensus interferon is a recombinant type 1 interferon that was derived by scanning sequences of naturally occurring alfa interferon and adding the most frequently observed amino acid in each corresponding position. As a result CIFN has much higher biological activity than pegIFN so it "adheres to the virus cell more tightly than pegIFN," said Dr. Kaiser. Dr. Kaiser said the study was investigator initiated and did not receive any industry support.
Primary source: Digestive Disease Week
Source reference: Kaiser, S et al "Comparison of Daily Consensus Interferon versus Peginterferon alfa 2a Extended Therapy of 72 Weeks for Peginterferon / Ribavirin Relapse Patients with Chronic Hepatitis C" Abstract S1060
Coping With Your Hepatitis C Diagnosis...
It's very likely that you have known that something wasn't "right" for a while. Perhaps you thought that you were just run down, out of shape or not eating well. On the other hand, you may have suspected the worst: could your symptoms be due to a tumor, or even cancer? Chances are that if you shared your concerns with family or friends they tried to reassure you. Maybe this helped, or maybe it didn't.
But now you are at the end of an extensive diagnostic process. Maybe you've had bloodwork, an ultrasound, or even a liver biopsy. And now your doctor has told you that you are infected with the Hepatitis C virus (HCV).
How do you feel? How are you supposed to feel? And what do you do now?
Understanding your Reaction...
Your new diagnosis is a life-changing event. You can expect to have a whole range of different feelings about it, feelings that may be uncomfortable and hard to predict. Some healthcare experts have applied Elizabeth Kubler-Ross' theory of grieving to help people understand their own reactions to their HCV diagnosis. Dr. Kubler-Ross' theory about the stages of grief, described in her 1969 book "On Death and Dying," was initially developed through her observations of terminally ill patients and their families. However, many mental health professionals believe that her 5-stage model can be applied to help people understand and possibly predict their emotional reactions to other events involving loss, such as loss of health, loss of relationships, loss of independence or even loss of employment. It's important to note that your progression through these stages is not rigid. People move back and forth between stages, and there's no timetable for how quickly one "should" move through the grieving process. Also, even though you may be the one with HCV, bear in mind that your diagnosis is going to touch the lives of everyone who cares about you. Your family and those close to you are going to have emotional issues to cope with, as well. In the Kubler-Ross model, the five stages of grief are denial, anger, bargaining, depression, and acceptance.
Denial
In the denial stage, one may simply not believe that the diagnosis is true. You may feel numb, or "in shock." Some people feel depersonalized, as though "it's happening to somebody else." You may feel nothing at all - for a while. Denial is not a bad thing - it helps one cope with feelings that may be overwhelming at the time, protecting the person from feeling out of control and helpless. As the shock wears off and you begin to accept the truth of your diagnosis, you will begin to experience other feelings.
Anger
In this stage, you've come to understood that your diagnosis is real and that you really have HCV, and you're angry about it. You may be angry in response to feelings of helplessness, or your anger may come from feelings that your diagnosis is "unfair." You may be angry at your own body or at God for "giving" you hepatitis. You may find yourself preoccupied with what could have been done to prevent the illness. You may also find yourself experiencing strong feelings of guilt as you struggle with the idea that you may have caused the disease can be difficult to cope with strong feelings of anger. You may be prone to lash out, or to "medicate" your feelings with alcohol, drugs or some other behavior. If you are the family member of someone with HCV, you may find the patient directing irrational anger at you.
Bargaining
As the anger subsides, you may find yourself trying to "make deals with God" to make your HCV go away. If this doesn't work, you may find yourself angry again, perhaps questioning and doubting your beliefs or spiritual relationships.
Depression
As bargaining subsides, the truth of your situation begins to "sink in." You may begin to have profound feelings of sadness and loss. Sleep disturbance, loss of appetite, lack of energy, poor concentration, and crying spells are common outward manifestations of depression. It is important to understand that this sort of depression is a normal part of the grieving process. However, depression that significantly interferes with basic activities (eating, bathing, dressing, etc.) or leads the person to thoughts of injuring themselves or others requires immediate (if not emergency) medical care.
Acceptance
Acceptance does not mean happiness. It means that you have allowed enough time and found enough support (from family, friends, or faith) to move forward in your life - your life as it is, not necessarily as you would like it - without suffering crippling emotional reactions or engaging in self-destructive coping behaviors.
Sometimes a "trigger" event will occur that will bring up strong feelings or anger of sadness months or years into the process. This can be something as small as a familiar smell or an old song.
Facilitating the Process
Coming to terms with your diagnosis is not easy, but there are some practical steps you can take to move ahead with your life: Give yourself plenty of time. Don't expect to come to terms with your diagnosis immediately. Learn all you can about HCV. Although Hepatitis C infection isn't rare, most people don't know much about it. As you learn about the disease, you empower yourself to make informed decisions about your care. Participate in a support group. Sharing your feelings and fears with other can decrease your feelings of isolation, and also provide practical advice for day-to-day coping. Use a journal to document your progress. If you tend to be obsessive, capturing your feelings and thoughts on paper can help you to "let go" and decreases anxiety.
If you are compulsively using alcohol, drugs, gambling, sex, or any other pusuit to avoid your emotions, stop. If you can't stop, get help.
Source: Hepatitis Neighborhood
Attention Hepatitis C Advocates

Attention Hepatitis C Advocates,
On June 7, 2006 the fate of hepatitis C prevention funding for 2007 will be decided by the U.S. House Appropriations Labor-HHS-Education Subcommittee. We need your help!
Your Representative needs to hear from YOU that hepatitis C funding is a priority. We cannot afford another year of flat or decreased funding. The House Labor-HHS-Education Appropriations Subcommittee is the panel that will decide funding amounts for hepatitis programs.
On June 7, 2006, the House Labor-HHS-Education Subcommittee is scheduled to decide critical funding needs for health programs - including hepatitis C. Silence on this issue will result in further cuts to an already precariously small hepatitis C allocation of $16.7 million for the Division of Viral Hepatitis (DVH) at the Centers for Disease Control and Prevention (CDC). A small increase of $10 million can make a big difference. The U.S. Senate will work on the their version of the bill in the coming weeks, however, a win now will move us one step closer to securing necessary resources for hepatitis C.
Contact your Representative NOW. We have about 8 days left to educate House Appropriators about the inadequate funding for hepatitis C programs.
WHEN: Right now! Your Representative needs to hear from you by close of business June 6, 2006.
Go to: http://www.democracyinaction.org/dia/organizationsORG/IMPACTC/campaign.jsp?campaign_KEY=4011
Thank you for your support.
Sincerely,
Lorren Sandt
Hepatitis C Caring Ambassadors Program
Managing Ambassador
877-737-4372 toll-free
lorren@hepcchallenge.org
Hepatitis C: Choices now on line at: www.hepcchallenge.org
"We believe strongly in the power of people working together, and that, by doing so, we will make far more significant advances than could be made by any group or discipline working on its own."